The Age Of Nasal Oxygen
Goal:
To explore the nasal Oxygen bridging methods to GlideScope intubation.
Recent developments highlight the safety of nasal O2 strategies in clinical airway management.
The Classic Methods of Nasal Oxygen delivery are:
1. Standard nasal cannula - delivers 20-40 % O2 to Patients breathing via the nose.
2. Reservoir cannulas - more efficient O2 delivery.
3. Venturi Mask - entrains air to deliver 24-40 % O2.
4. Simple Face mask- delivers 40-60 % O2 at a flow of 5-10 L per min.
5. Non Rebreathing Tight fitting facemark with one way valve- delivers 40-90% oxygen @ 8L
6. Naso-tracheal cannulas - humidified and lower flows .
7. Naso-pharyngeal cannulas with low flow.
State of the Art Nasal Oxygenation strategies:
2 new forms of Nasal oxygenation are now proven to provide extraordinary advanced nasal Oxygen capability.
I Nasal TsePAP
{kind=link}
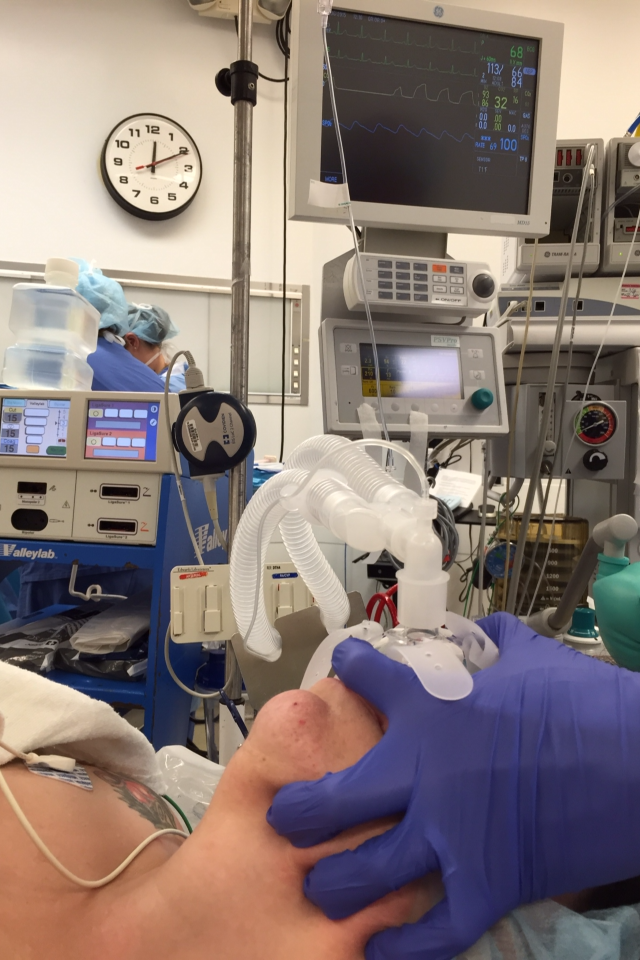
The comprehensive new technology advocated by Dr James Tse from Rutgers University represented by use of nasal CPAP is suited and proven to maintain excellent oxygenation during GlideScope Intubation and during MAC anesthesia or conscious sedation. The advantage of this strategy is that the Nasal TsePAP airway uses the proven advantages of the Nasal approach while the patient may be in a variety of positions which can accept a temporary positive pressure intervention if required without any adjustment of the equipment. Detail on the use of this technology will follow.

Photo: GlideScope intubation with Nasal TsePAP mask in place
Courtesy of Dr. James Tse
II High Flow Nasal Oxygen
Anil Patel and S Nouraei have shown (1.) that apneic patients can be maintained for extended periods of time up to 16 minutes by use of Very high flows of nasal humidified Oxygen. Obesity significantly reduced the effectiveness to the 5-7 min range of time above 90 O2 SAT in some patients.
Patients were 40 degrees head up and had 70 L per min. of humidified O2 delivered through the Optiflow delivery system.
No comments:
Post a Comment